Plantar fasciitis - a pain in the arch!

Dr Terri Bidwell (Orthopaedics) & Dr Chris Hanna (Sports Medicine)
June 4, 2018 SharePlantar fasciitis is a pain on the bottom of the heel +/- the arch of the foot
Important underlying factors include a lack of strength and mobility around the foot and ankle which causes overload of the plantar fascia
Treatment of the condition is successful when combined with appropriate activity modification and addressing the underlying causes
10% of runners will get plantar fasciitis. It is useful to have some understanding of the anatomy, pathology and biomechanics of this condition. This will help you a) avoid it or b) recognise it, seek help and make the necessary changes to avoid chronic injury.
What is the plantar fascia?
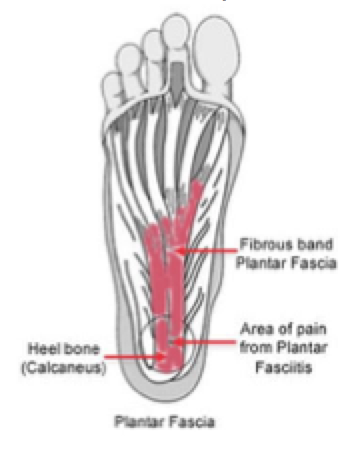
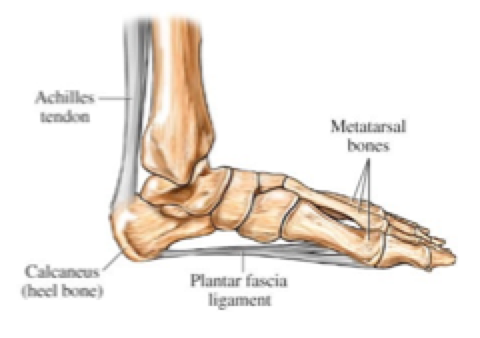
The PF is a layer of thickened fibrous tissue that runs along the bottom of the foot under the skin and fat. It is attached to the undersurface of the calcaneus (heel bone) and splits distally to connect with all 5 toes. It is the thick central band which is usually involved.

The plantar fascia strengthens the arch of the foot - similar to a tension bridge underneath the arch. It is part of the shock absorption mechanism of the foot. The vertical forces it has to absorb during foot strike can be several times bodyweight.
 When the attachment of the plantar fascia to the calcaneus becomes overloaded, pain is felt on the sole of the foot underneath the heel and /or along the arch. This is often noticeable in the mornings on the first few steps getting up. Morning pain is a hallmark symptom. It also occurs after running or after long days on your feet especially if surfaces are hard or shoes are inadequate. It is important to note that there are other causes of heel and foot pain (such as lateral plantar nerve entrapment, calcanea stress fracture and achilles insertion problems) so it is worthwhile having the diagnosis confirmed by a professional. Pain behind the heel is also likely to have a different cause.
When the attachment of the plantar fascia to the calcaneus becomes overloaded, pain is felt on the sole of the foot underneath the heel and /or along the arch. This is often noticeable in the mornings on the first few steps getting up. Morning pain is a hallmark symptom. It also occurs after running or after long days on your feet especially if surfaces are hard or shoes are inadequate. It is important to note that there are other causes of heel and foot pain (such as lateral plantar nerve entrapment, calcanea stress fracture and achilles insertion problems) so it is worthwhile having the diagnosis confirmed by a professional. Pain behind the heel is also likely to have a different cause.
Inflammation or degeneration?
Historically it was thought the pain was inflammatory in nature. The actual nature of the problem is now better understood. There is repeated micro trauma to the attachment area. This is caused by repetitive overloading that exceeds the ability of the body to repair the damage. The tissue becomes disorganised and there are areas that lack adequate blood supply. It is more like a chronic degenerative condition than an inflammation.
Causes
Some people have underlying anatomy which predisposes them to irritation of the plantar fascia. This includes those with high arched feet as well as those with flat feet.
However, the main issues which are thought to trigger PF in runners are lack of joint mobility and weak muscles (yes, the very same factors that contribute to many other injuries!)
Strength and Mobility
Weak calf and foot muscles overload the plantar fascia. In particular “lazy” small muscles to the toes means more force on the fibrous plantar fascia.
Lack of ankle dorsiflexion is strongly associated with plantar fascia strain. If you can’t do a low squat without your heels coming off the ground, you probably lack mobility due to tight calf muscle/tendo achilles and ankle joint structures. This can be improved by mobility and stretching exercises and for women, avoiding prolonged use of high heels.
Diagnosis and prognosis
It is important to get a diagnosis from a qualified health professional to exclude other conditions and access the best information and treatment. Plantar fasciitis rarely needs invasive treatment such as surgery but can be very difficult to resolve with symptoms lasting as long as two years or more. Appropriate rest and addressing the underlying issues can shorten the duration of symptoms and prevent recurrence.
Treatment
Of the numerous treatments described, the most useful are:
Rest and activity modification
For any treatment to be effective it needs to be accompanied by reduction of the aggravating activities. Unfortunately this means running…especially up hills. This is easier to stick to if it is replaced by non aggravating exercise. There are a lot of options here but in particular it is worth noting that runners have been able to substitute a month of on land run training with aquatic running with no detriment to performance (including factors such as VO2 max and ventilatory threshold). Another study has shown 30% of run volume van be replaced with aquatic running for a 6 weeks period with no change in performance. The addition of aquatic running has been shown to actually improve run performance in some people. This is well worth considering if you are training for an event in the near future.
Physiotherapy
Addresses the underlying biomechanics factors of poor mobility and muscle weakness. Exercises to increase ankle mobility especially ankle dorsiflexion are particularly useful in those people who have poor dorsiflexion. Stretching of the plantar fascia in addition to the calf muscles has been shown to be even more effective than either alone.Strengthening of the calf muscles and very importantly the small muscles of the foot will reduce load the plantar fascia. The physio may prescribe a towel scrunching exercise - where a towel is scrunched up under the bare foot.
Night splints
These are light calf-foot orthoses that hold the ankle in at 90 degrees during the night. This stops the tightening of the calf/tendoachilles and ankle joint that occurs at night when the foot lies plantar flexed (pointed downwards) during sleep.
They improve early morning pain and control overall symptoms. some people find these more acceptable than others. If you can stand wearing them, they will probably help.
Orthotics
Are helpful in some cases especially to support the arch and mechanically reduce the strain on the plantar fascia. over time, as the foot muscles strengthen these would ideally become unnecessary. They are well worth considering in the acute phase and a podiatrist would likely be helpful here.
Shoes
Shoes (or lack of them) do matter. It is very difficult to make any direct evidence based global recommendations. For example, barefoot/minimalist running has cured plantar fasciitis in some individuals, probably because it encourages the strength and mobility of the foot and ankle joints and the surrounding musculature. However, too much minimalist running in a non conditioned athlete can cause plantar fasciitis and be particularly aggravating.
In terms of running shoes it seems to be a question of trying different things and using what works. This seems to be a cushioned shoe for many people.
The only firm recommendations are the use of more cushioned shoes for those on their feet all day at work and minimising the time spent in high heels for women.
ESWT (Shockwave therapy)
Extra-corporeal shockwave therapy is available through sports medicine clinics. An ultrasound probe is used to deliver shock wave impulses. It is non invasive. The treatment reduces pain initially by changing the behaviour of the nerves in the area. It also produces a regenerative “tissue healing” effect in the area being treated. this is especially helpful where poor blood supply is part of the problem, like it is in the plantar fascia insertion.
ESWT has been shown to be effective in treatment of plantar fasciitis and is FDA approved for this condition.
Invasive treatments
More invasive treatments including injected steroid and surgical treatments are available. These are unnecessary in most individuals and have risks of complications which can be quite significant. These would be best discussed with a person’s own specialist.
Summary
A major cause of plantar fasciitis is an athlete being insufficiently strong and mobile for the loads they are placing on the calf-ankle foot. This can occur due to a rapid increase in distance or load increases caused by hill running or jumping exercises or other training errors. Treatments are available to treat acute symptoms. The most promising of these is ESWT which is available through Sports Medicine clinics. Treatment will be most effective if it is accompanied by an in initial reduction in aggravating activities (rest/cross training until acute symptoms resolve) and a focus on improving strength and mobility.
- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -
 Terri Bidwell has extensive experience as an endurance athlete. She has run over 50 marathons and many Ultramarathons, including the legendary Marathon des Sables stage race. She has raced paddle boards, taken part in marathon open water swimming events and is a 4x Ironman Triathlete (and two-time Kona qualifier.) She holds Science & Medicine degrees (BHB, MBChB 1996 Auckland ) and has been in specialist practice as an orthopaedic surgeon for 10 years. She has twice been Race Doctor at Ironman Hawaii and is a regular on the medical team for the Tarawera Ultramarathon.
Terri Bidwell has extensive experience as an endurance athlete. She has run over 50 marathons and many Ultramarathons, including the legendary Marathon des Sables stage race. She has raced paddle boards, taken part in marathon open water swimming events and is a 4x Ironman Triathlete (and two-time Kona qualifier.) She holds Science & Medicine degrees (BHB, MBChB 1996 Auckland ) and has been in specialist practice as an orthopaedic surgeon for 10 years. She has twice been Race Doctor at Ironman Hawaii and is a regular on the medical team for the Tarawera Ultramarathon.
Terri will be contributing a series of articles on medical/injury matters for Wild Things. Thanks Terri!